
Online talk “What’s In Your Kit” (WYIK): 3rd June 2021 @ 7pm NZST
June 1, 2021
Society Incorporation, formal memberships and caps for sale!
July 26, 2022
(This post was originally published by dr Malin Zachau on her personal website. It is republished here with permission.)
To those of you who attended the SAR day on Tuesday 25 May 2021 in Wanaka, many thanks for being enthusiastic , engaged and friendly groups to work with.
Some of you asked if the content would be on my website , normally I would post references etc in advance but I simply did not have time to do so but here we are, better late than never, right?
Determination of death in mountain rescue (ICAR 2020) this is the link to the open access, full text that my work shop was based on. (Please be advised there are some very graphic photos in the article). The audience on the day was predominantly search and rescue volunteers, (LandSAR New Zealand) ski patrollers, mountain guides, other snow industry. There were also a few professional SAR (NZ Police), an intensive care flight paramedics and a couple of doctors.


From left to right: Dr Robin Barraclough (he delivered a separate AvaLife workshop), Aleksandra Pawlik, me with my flash new portable public address system and Dany Freestone.
The workshop would not have been possible without the help of Aleksandra and Danny facilitating the individual patient scenarios, and I’m very grateful to them for their enthusiasm and support. The workshop would not have been possible without the help of Aleksandra and Danny facilitating the individual patient scenarios, and I’m very grateful to them for their enthusiasm and support.
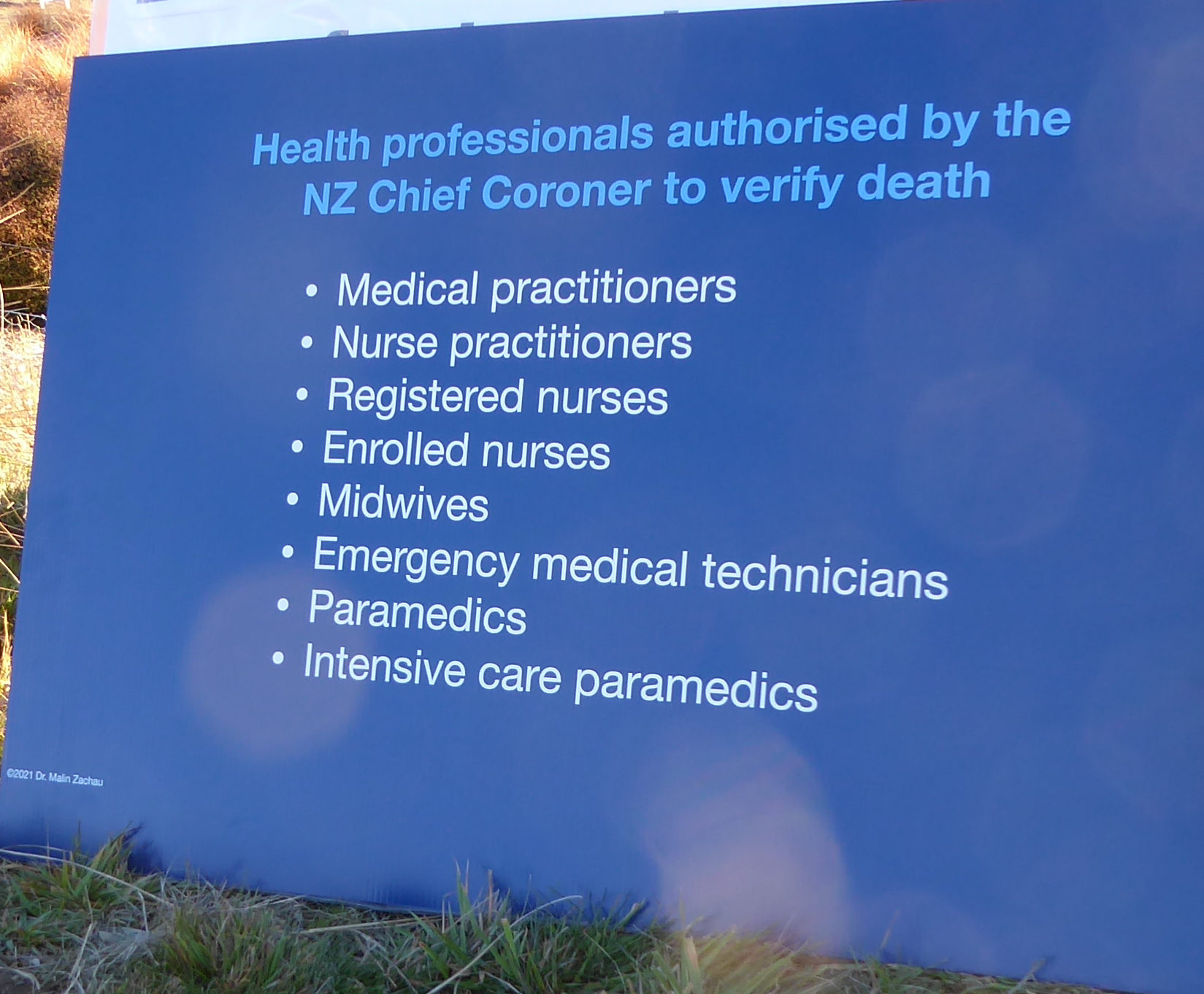
My first 90 by 60cm corflute sign was to draw everybody’s attention to the fact that in New Zealand SAR volunteers, professional SAR practitioners or mountain guides are not legally authorised to verify (determine) death. On the white corflute (ICAR recommendation flowchart) the circumstances under which it might become necessary: scarcity of resources, unacceptable risk for rescuers, extreme environment , mass casualty situations. However, if none of those exist and there is any uncertainty at all about the signs of death, then the legal authority to determine death does not exist in NZ for SAR volunteers.

The SAR day consisted of 5 workshops, each lasting one hour, and circulated though in a “round robin” fashion , thus we delivered this workshop 5 times. We were super lucky with the weather, the morning started off about 4*C and after lunch when the sun came out it felt much warmer than the 12*C it was. We had two scenarios in this workshop, each had a manikin kindly lent to us by Trevor Hunter of Laerdal NZ and Robins AvaLIfe workshop also had 5 of Trevor’s Laerdal QCPR manikins.



One scenario was “Bob the butcher” who had been reported overdue by his wife following a solo day tramp. Bob was a good friend to everyone in the “simulated SAR team” that found him. Bob had sustained a significant traumatic brain injury with a large part of brain exposed but without having lost a significant amount of brain matter. Different groups reached different conclusions regarding the care of Bob, some taking into account that they had an emotional attachment to him, whereas other groups entirely overlooked that aspect. Some rescuers recounted lived experiences of incidents where friends had died. I mentioned that psychological injury in rescuers was going to be the topic of my “the elephant in the room” presentation at the SHAC conference two days later. Some groups elicited that Bob has rigorous mortis, other did not. Overall, it made for very useful discussions during the debrief and I hope everybody learned something, even if it is just to double check with their own organisations what their standard operation procedures are since they should only withhold active resuscitation if there is no shadow of a doubt about the non- viability of the patient. Some groups were rather too cavalier with determining that Bob was dead without establishing whether or not he had rigor mortis or dependent lividity.

The other scenario was Kim, the instagram influencer ( extreme intermittent fasting) from Auckland who was overdue after a day tramp. She was unsuitably dressed for the overnight temperature and had become cold. She was unresponsive and different groups found different vital signs. Being a “smart manikin” her respiratory rate was 4 per minute ,her pulse was 15 per minute, her pupils were dilated and un-reactive. Some groups found that she was breathing very slowly and realised she was hypothermic and requested evacuation. Other groups did not find her breathing and started CPR, again realising that she was hypothermic. Both of those management were considered correct and simply highlighted how difficult it can be to find a very slow respiratory rate. No group determined that she was dead, which was great because if they had done so Danny who facilitated the scenario was ready to make the Resusci Annie (Kim) manikin scream which would have taken the participants by surprise!
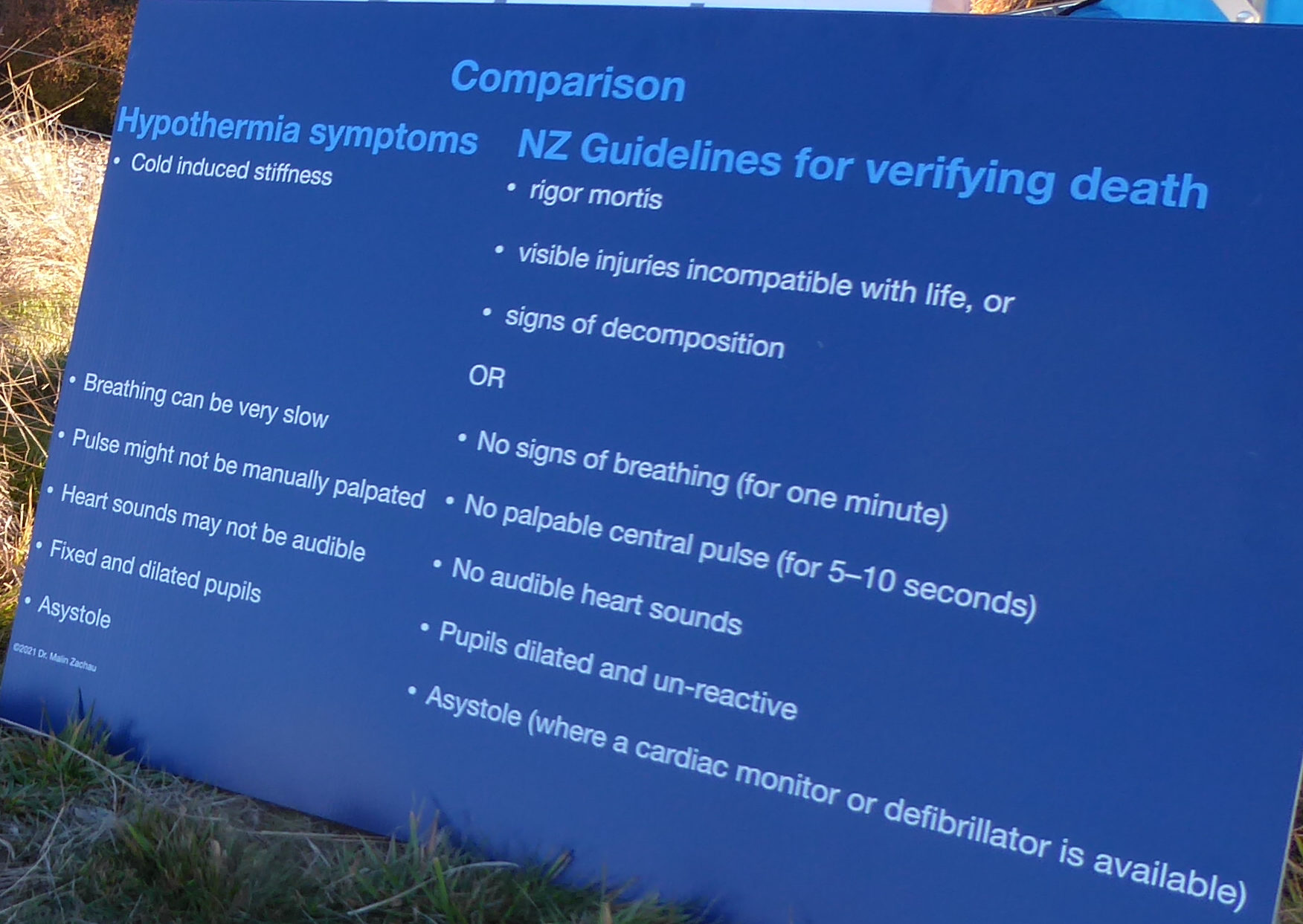 The scenario of Kim elicited lively discussion during debrief and I explained that in New Zealand it is quite possible for a health care professional to verify a patient dead when they are actually just cold, due to the criteria required by NZ Ministry of Health. In some other countries a certain core body temperature is necessary before a patient can be verified dead ( 33 and 35*C respectively in Sweden and the UK ). I mentioned that maybe we need to get that changed here in New Zealand but in the meantime, hopefully increased awareness amongst rescuers first on scene will help to avoid errors.
The scenario of Kim elicited lively discussion during debrief and I explained that in New Zealand it is quite possible for a health care professional to verify a patient dead when they are actually just cold, due to the criteria required by NZ Ministry of Health. In some other countries a certain core body temperature is necessary before a patient can be verified dead ( 33 and 35*C respectively in Sweden and the UK ). I mentioned that maybe we need to get that changed here in New Zealand but in the meantime, hopefully increased awareness amongst rescuers first on scene will help to avoid errors.
All the groups engaged really well, were able to suspend disbelief , the scenarios were well received and I believe they met the goal which was to start the discussion on this crucial topic.


{kind=link}
{kind=link}